
Fingers 101
Anatomy & Function
-
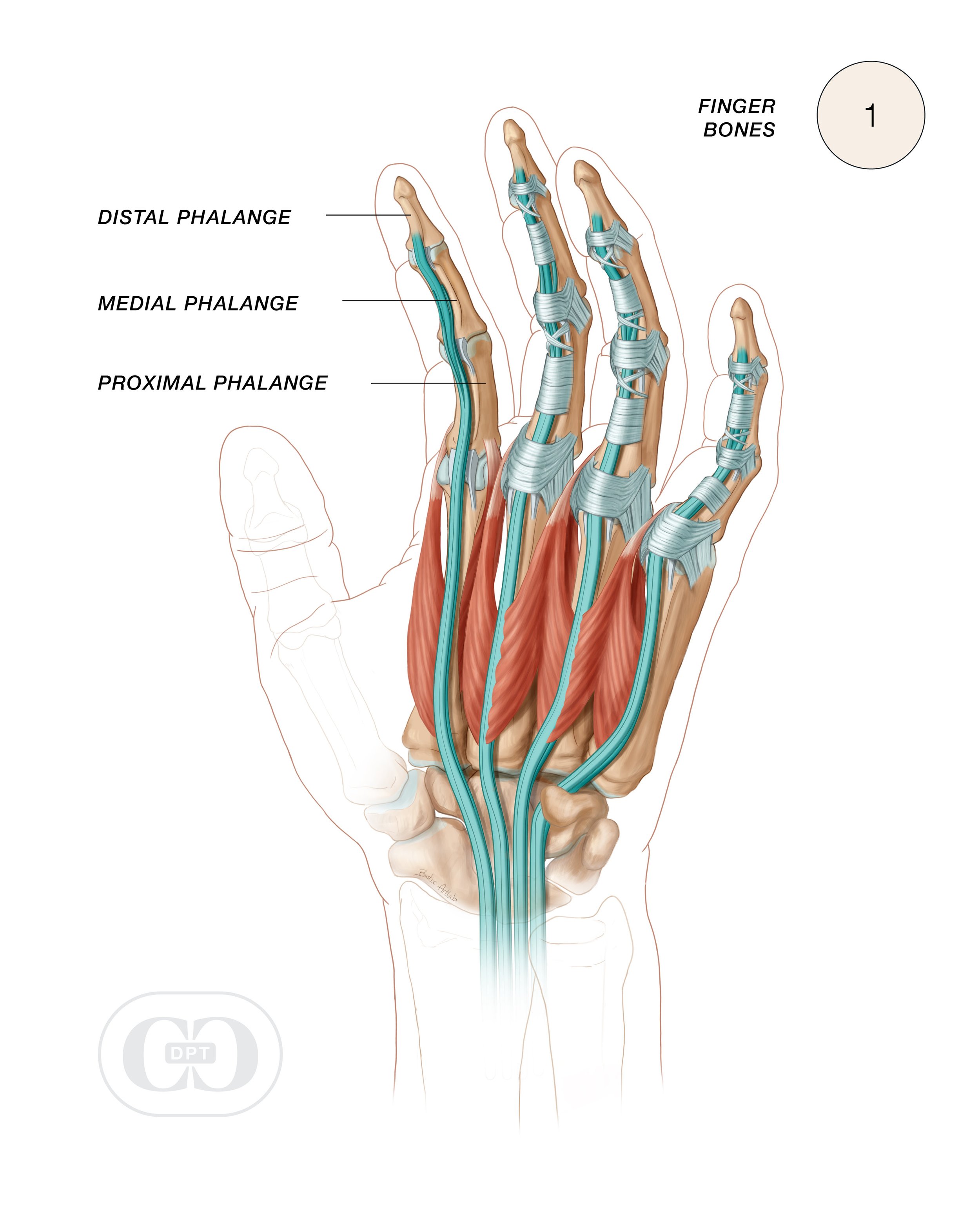
To better understand finger injuries in climbers, there are several important structures within the four (non-thumb) fingers that are important to get acquainted with (See Fig. 1).In order to understand what’s going on with your injury, there are a few important structures within each of the four fingers you need get acquainted with first (excluding the thumb).
Three bones
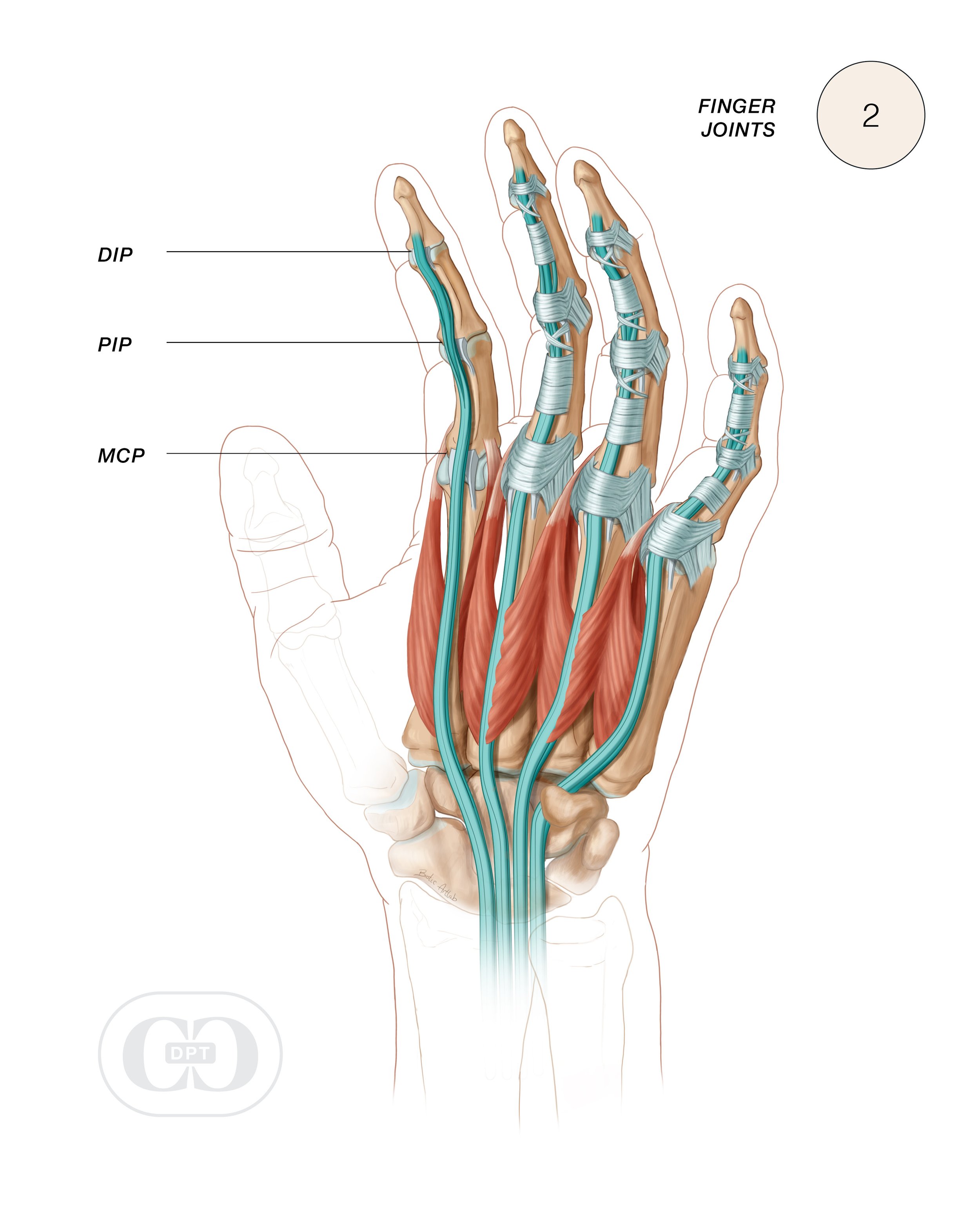
Three joints: Joints are where two bones articulate. In each finger, there is a metacarpalphalangeal joint (MCP), proximal interphalangeal joint (PIP), and distal interphalangeal joint (DIP).
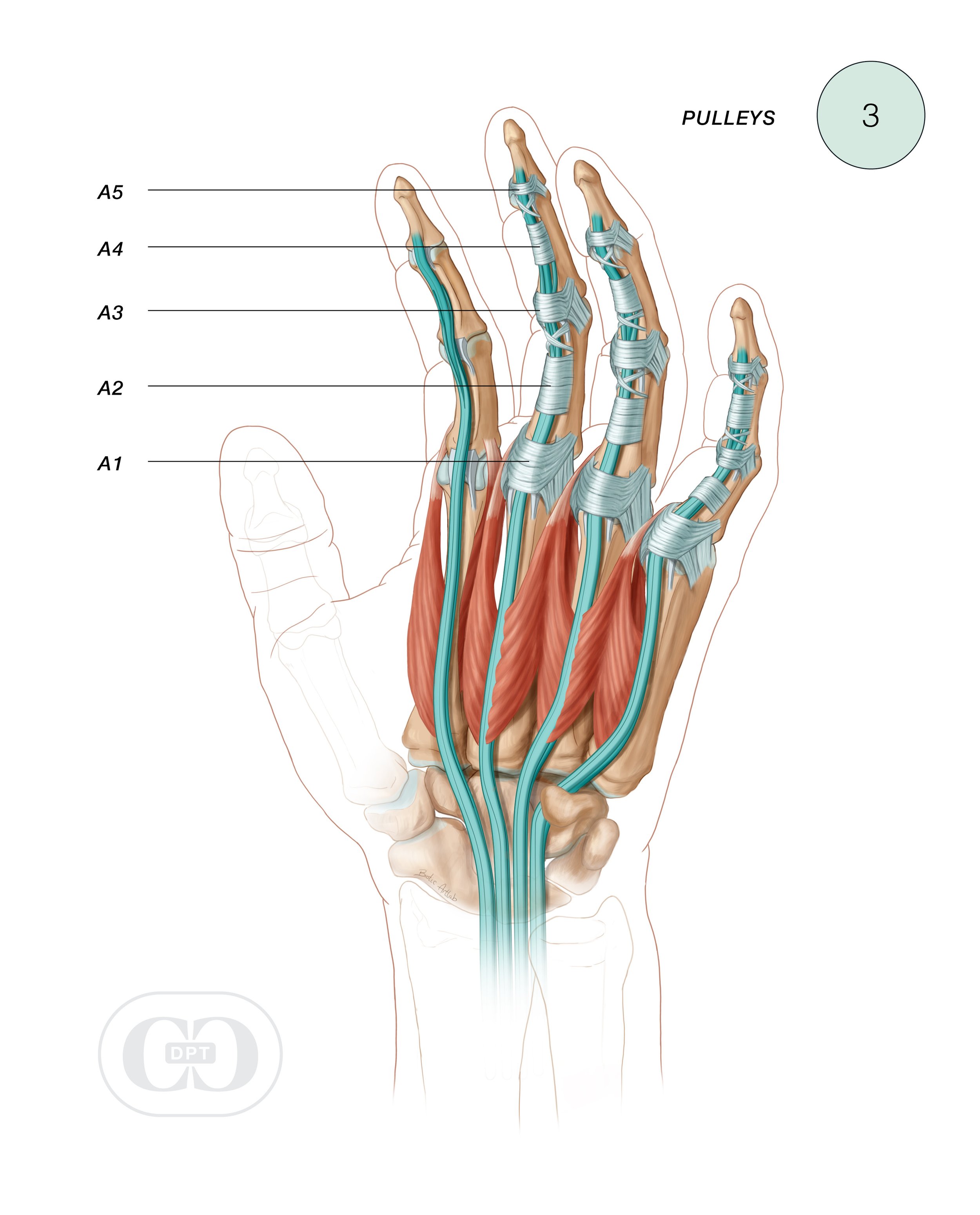
Five pulleys: A1, A2, A3, A4, A5. Each of the four fingers has all 5 pulleys, and their location is the same on each finger.
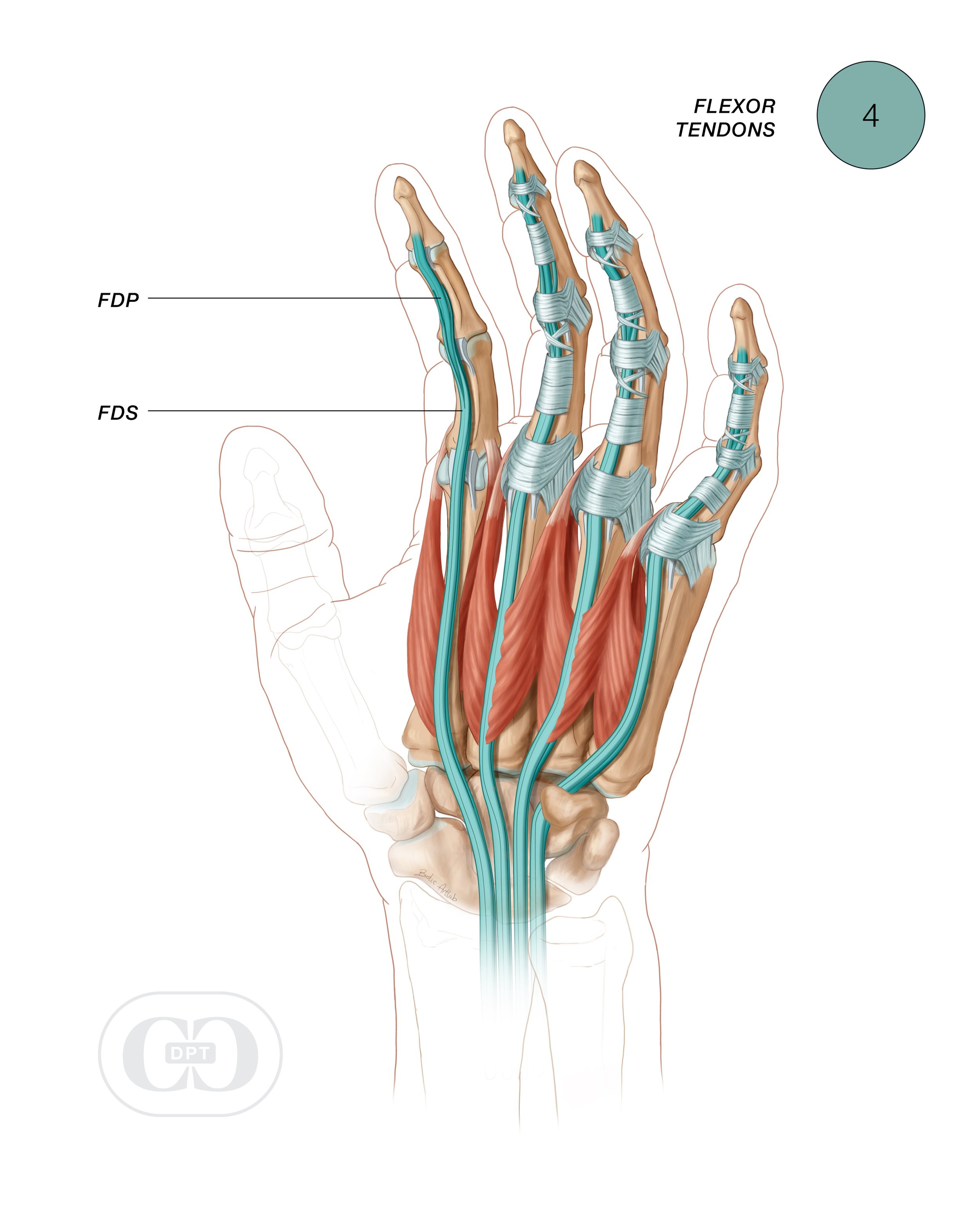
Two flexor tendons: The muscles of these tendons are located in the forearm, but the tendons insert on the fingers and move the fingers. Each flexor is one muscle that actually moves 4 fingers, so you don’t have a separate flexor muscle for each finger, but you do have separate tendons. They are called the Flexor Digitorum Superficialis (FDS), and the Flexor Digitorum Profundus (FDP). The FDP pierces through the center of the FDS prior to its insertion on the distal finger bone.
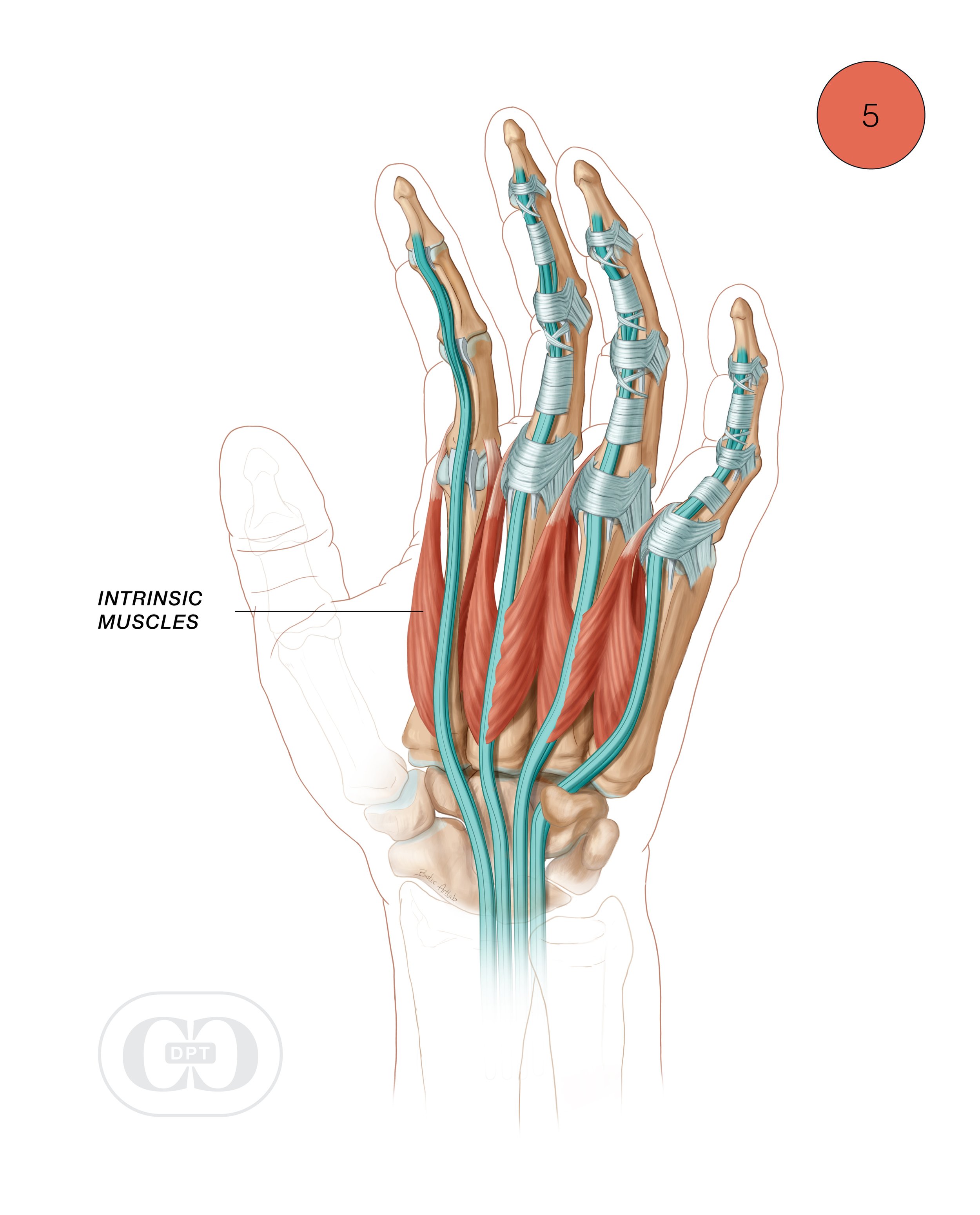
Hand/finger intrinsic muscles: These muscles are located primarily in the hand, but they insert on the finger bones and guide finger motion and finger position. They are known as the lumbricals and the interossei muscles.
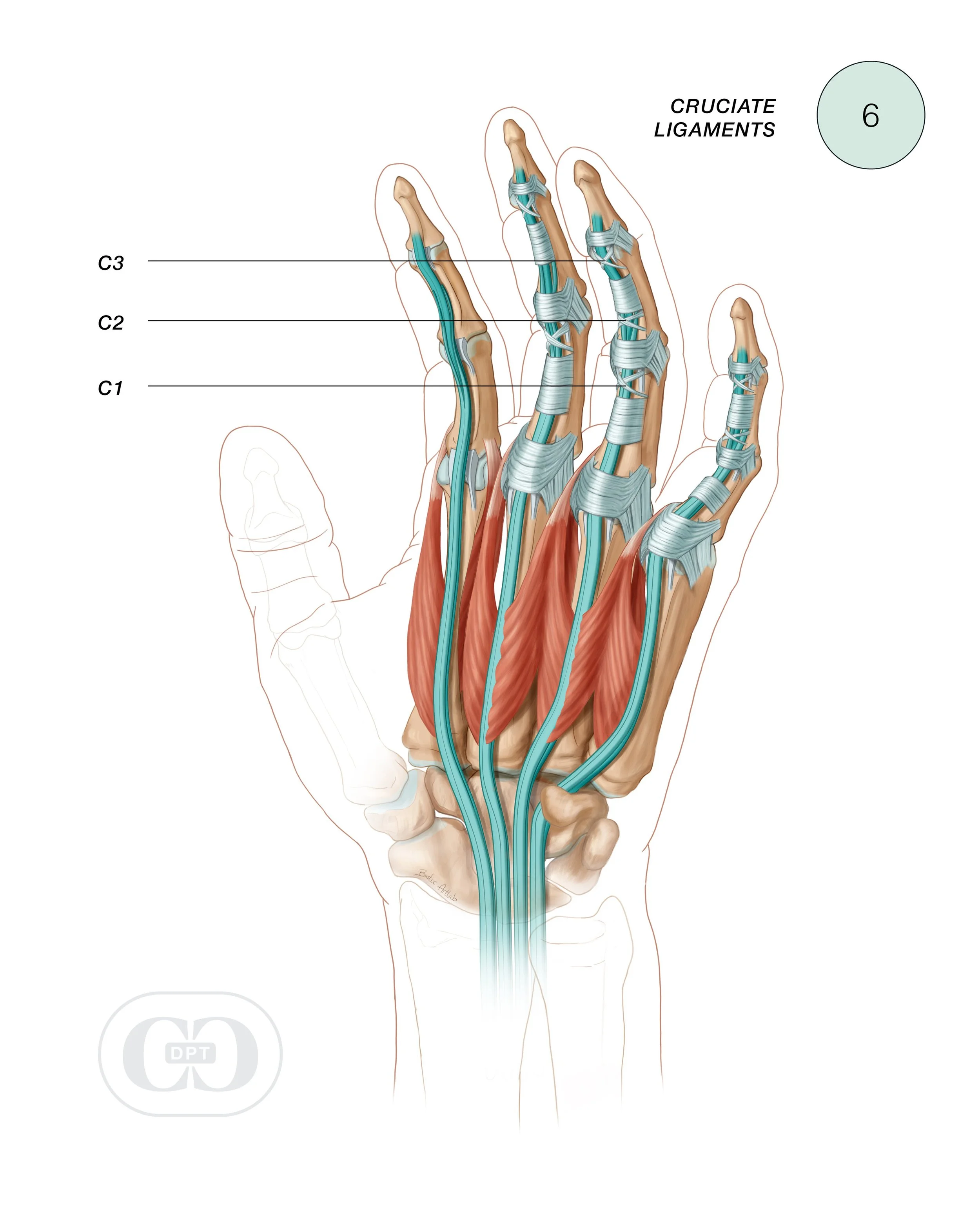
Three cruciate ligaments: These ligaments are in an “X” pattern, and are located between a pulley and a joint on the path down the finger.
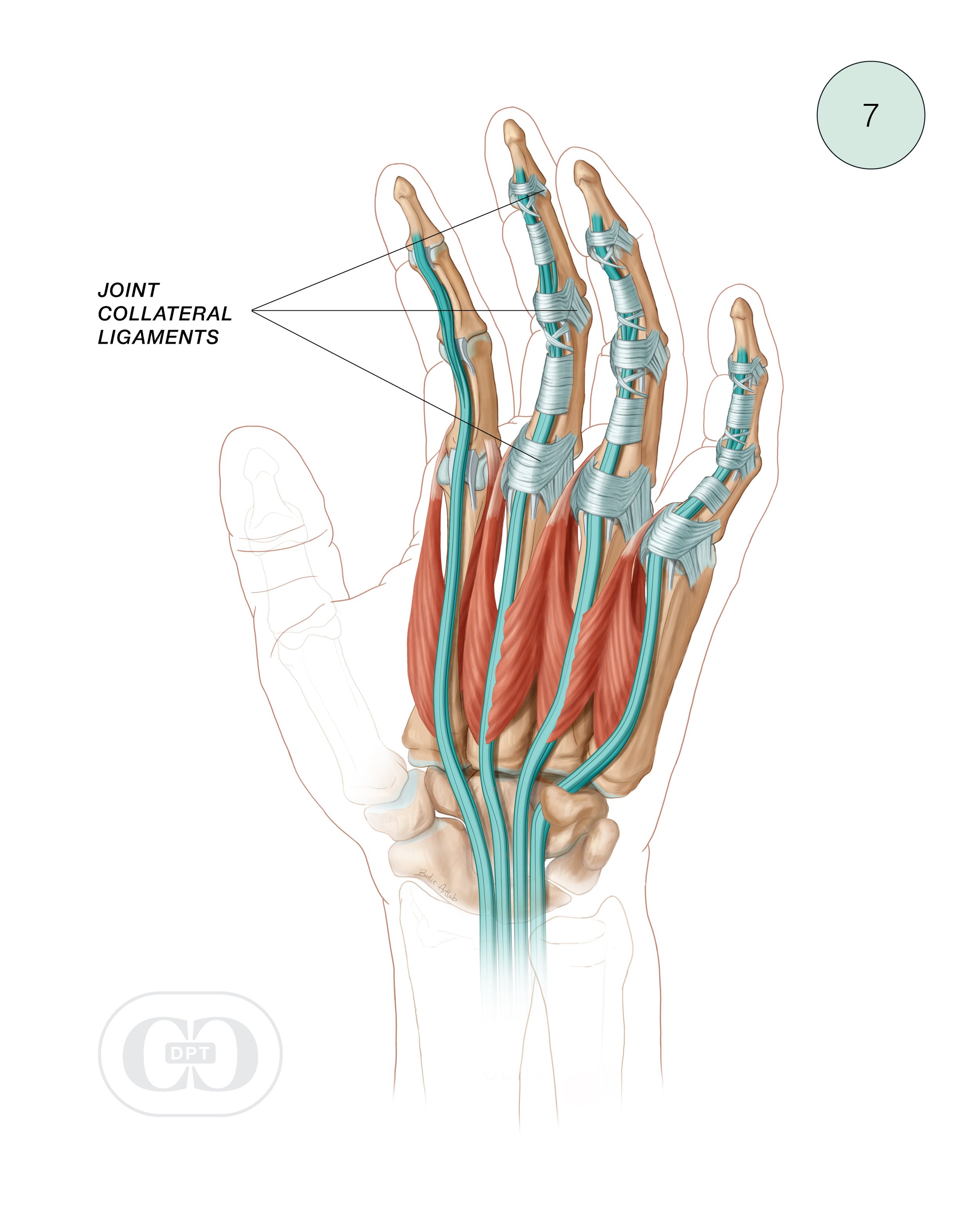
Joint collateral ligament: Collateral ligaments stabilize the sides of each joint.
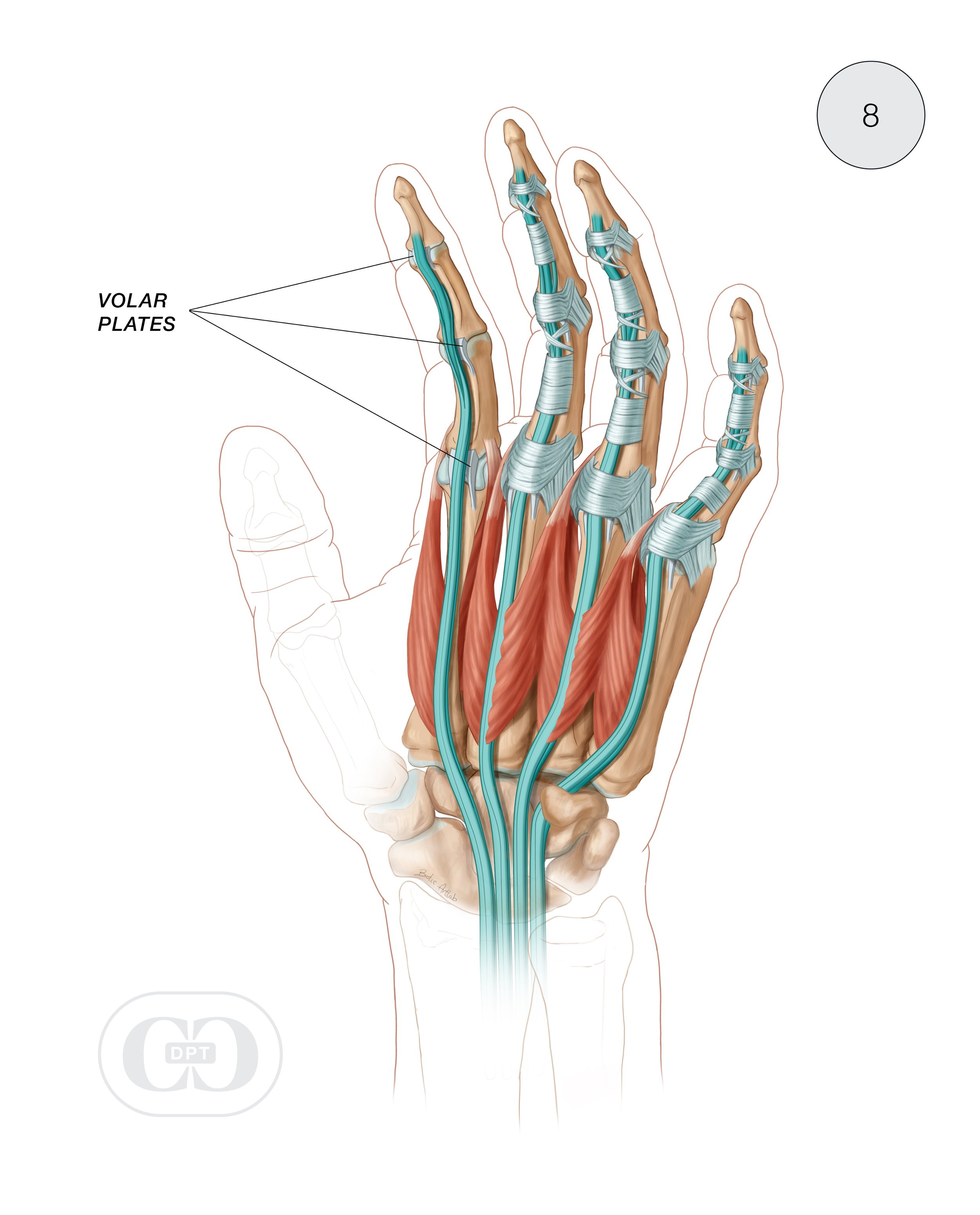
Volar plates: These are stabilizing ligaments located on the volar side of each joint of the fingers.
Joint capsules: The capsule is like a bubble of connective tissue that surrounds the joint. (Not pictured in diagram)
-
The finger flexor pulleys are transverse retinacular tissue structures that hold the flexor tendon unit to the bones of the fingers at 5 different points.
They act to mitigate forces of load through the finger to allow for finger flexion under resistance across the 3 finger joints. The estimated forces acting on pulleys vary depending on the hand position, hold size, and pulley location.
When a pulley is compromised, bowstringing occurs. Bowstringing refers to the excess in distance between the flexor tendon(s) and the bone. There are norms by which clinicians and researchers compare a given finger’s Tendon-Bone-Distance (TBD) and use it as an indicator that a pulley has been compromised. The bigger the TBD, the harder it is to bend the finger and function decreases.
-
Each finger joint, or Interphalangeal joint has a fibrous joint capsule that encapsulates the joint. The inner lining of the capsule is comprised of a synovial membrane. The synovial membrane provides fluid for lubrication of the joint, reducing friction while the joint in is motion. Each joint capsule is reinforced on the sides of the joint by the collateral ligaments and a palmar ligament, called the volar plate. Dorsally, the joint capsule is strengthened by a broadening of the extensor tendons called the extensor hood. The outer fibrous tissue of the capsule is often what is injured when you have a sprain of a joint. It can also become irritated and cause something known as Capsulitis.
In Climbing
Knowing the likelihood of certain injuries, their etiology and how to differentially diagnose is paramount to the timely treatment of these injuries. The most common injury in climbing is an A2 pulley strain. (Not surprising if you consider what we do with our hands.)
-
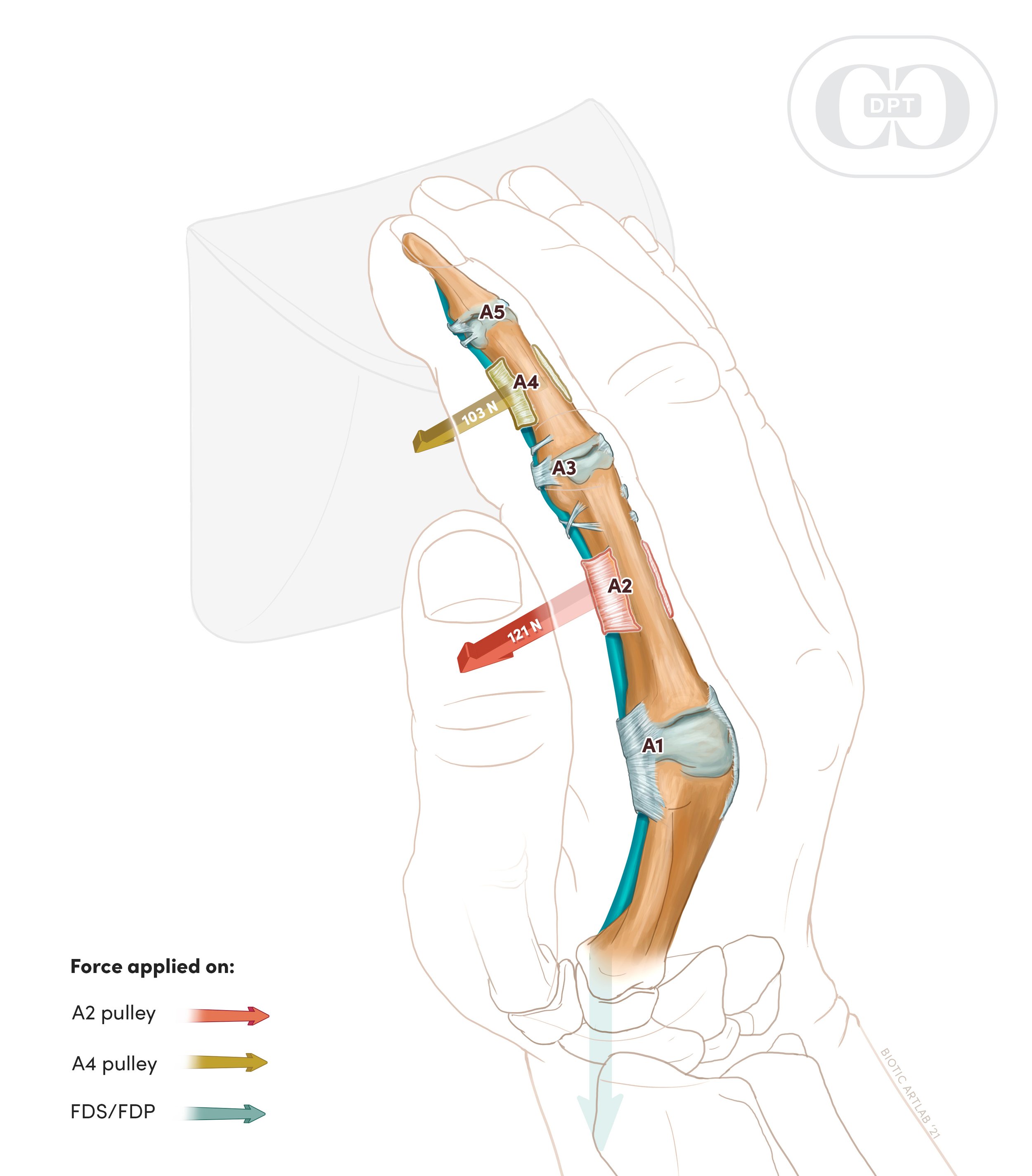
The flexor tendons cross many joints. Because of this, they need connective tissue that holds them to the bone and acts like a fulcrum for force production. Each pulley is positioned at a different point along this long line of tendon pull.
(Fig 2A) The Open Hand or Slope grip position is relatively safe for a healing A2 pulley, in that the force placed on the A2 during active flexion in an open hand position is far less than it is when the finger is in a full crimp position or even half crimp.
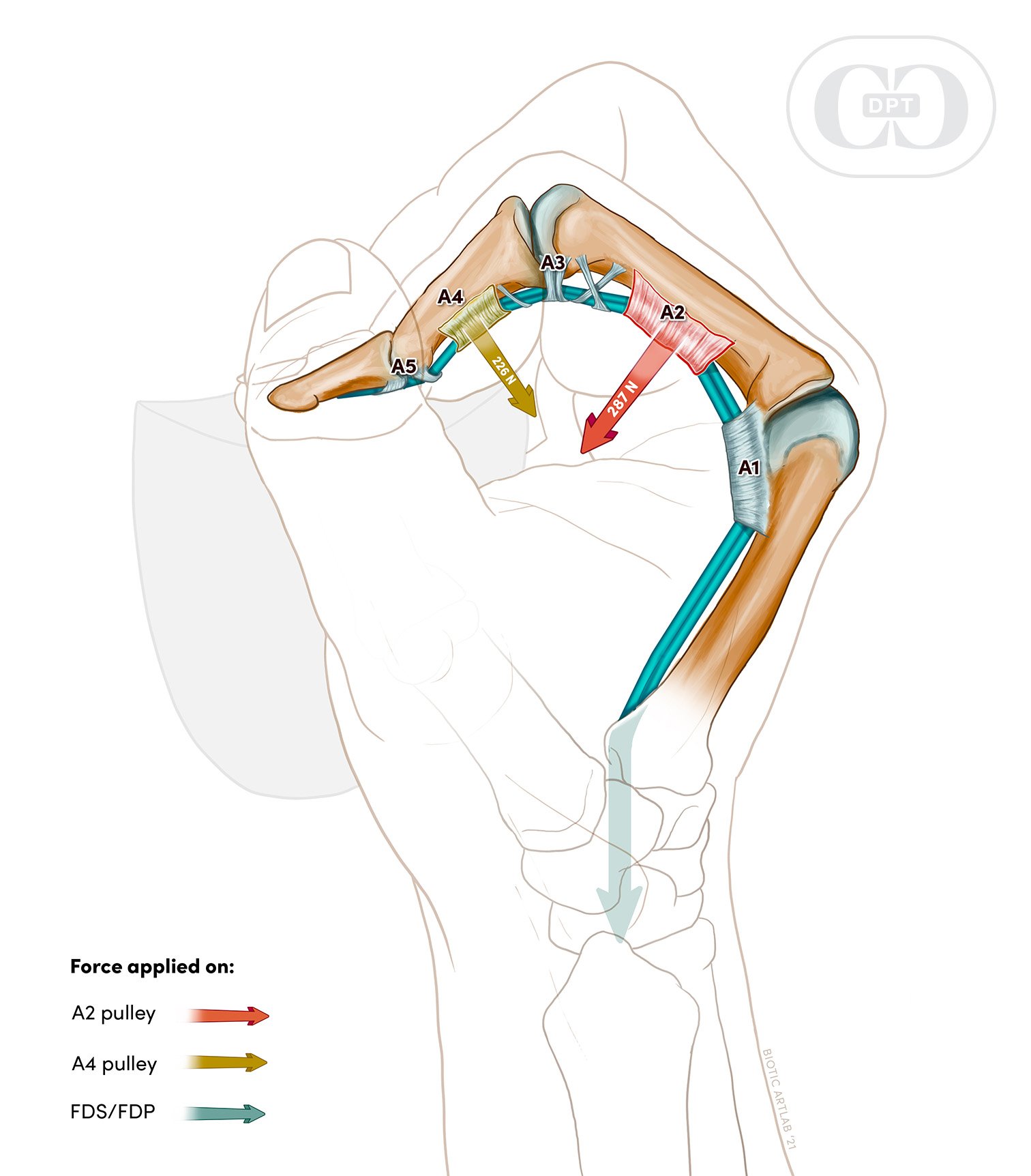
(Fig 2B) The full crimp position puts the greatest amount of force through the A2 pulley. This is why it gets injured more than any other pulley.
-
1988-90: First A2 pulley case study discussing prevalence, grips effected, bowstringing.
1999: Ultrasound for Pulley Injury Diagnosis and depiction of injury.
1988-90: First A2 pulley case study discussing prevalence, grips effected, bowstringing.
1999: Ultrasound for Pulley Injury Diagnosis and depiction of injury.
2000: Circumfrential Taping is shown to be an ineffective method for preventing pulley injury.
2001: Biomechanics of grip positions and forces acting on the pulley tendon complex.
2003: Schoffl Pulley Classification: Schoffl et al published the first diagnostic and therapeutic guideline for pulley ruptures after prospectively evaluating 604 climbing finger injuries — a seminal work for approaching pulley injuries.
2003: Trend toward looking at the biomechanics and the forces placed on climbers hands.
2007: H-Tape: Research shows this new taping strategy supports A2 pulley healing
2016: Pulley Protection Splint shown to heal ruptures of the A2 pulley
2020: Cooper Classification introduced conservative Tests and Measures for grading pulley strains and rehab for single pulley rupture
-
Publicly Available research!
Frolich, et al. (2021) Long term evolution of soft tissue response in the fingers of high-level sport climbers: A cross-sectional 10 Year follow-up study. Physical Therapy In Sport, 52, 173-179.
Cooper, C., & LaStayo, P. (2020). A potential classification schema and management approach for individuals with A2 flexor pulley strain. Journal of Hand Therapy, 33(4), 598-601.
Grip Repertoire
-

Full Crimp
No one has the same method of full crimping, but the general position is with the hand in its most closed position while keeping pressure on the tips of the fingers.
The technical explanation: MCP joints are in 60 degrees or more of flexion, PIP joint is in 90 degrees or more flexion, DIP joint is in neutral-extension.
-

Half Crimp
A half crimp position is simply a crimp with the palm flat or “open”. This position is often misidentified: climbers often claim they are in a half crimp when they are actually in a full crimp minus the thumb. This is probably the most difficult position for people who are very strong full crimpers to achieve.
The technical explanation: relative neutral MCP joints, PIP joints bent from 110 degrees flexion to 80 degrees flexion.
-

Open Hand
An open hand grip can be defined as when the palm is flat-ish and fingers are straight-ish.
The technical explanation: MCP joints in relative neutral, PIP joints in less than 80 degrees of flexion, DIP in relative neutral or any bend available.
-

Sloper
A sloper grip is uses an open hand while maintaining the maximum amount of skin friction being applied to a hold. Often the thumb squeezes the hold wherever possible to improve friction and grip.
(Note: just because the hold is a sloper, it doesn’t mean the grip being used is a sloper. Many people use a full crimp grip on sloper holds.)
-

Pocket
A pocket is a hold whose depth and width is only large enough for one to three fingers to grip. Usually, it’s a two finger pocket or a mono (one finger only).
-

Pinch
A pinch involves a grip position where the fingers are on one side of the hold while the thumb creates compression on the other side of the hold.
Evaluation Basics
-
Based on the 2003 diagnostic and therapeutic guideline published by Schöffl et. al., pulley injuries are typically classified into one of the following categories:
Grade I: Pulley strain (exhibits stretching or slight tearing)
Grade II: Partial rupture of the A2 or A3 pulley, or complete rupture of the A4 pulley
Grade III: Complete rupture of the A2 or A3 Pulley
Grade IV: Multiple complete pulley ruptures, requires surgical repair
-
This is the most effective way to accurately evaluate a pulley injury, as it uses high-frequency sound waves to produce images of the internal structure of the finger that allows a practioner to definitively measure the distance between the tendon and the bone. For when this method isn’t available, we’ve developed a new classification criteria to help evaluate A2 pulley injuries.
-
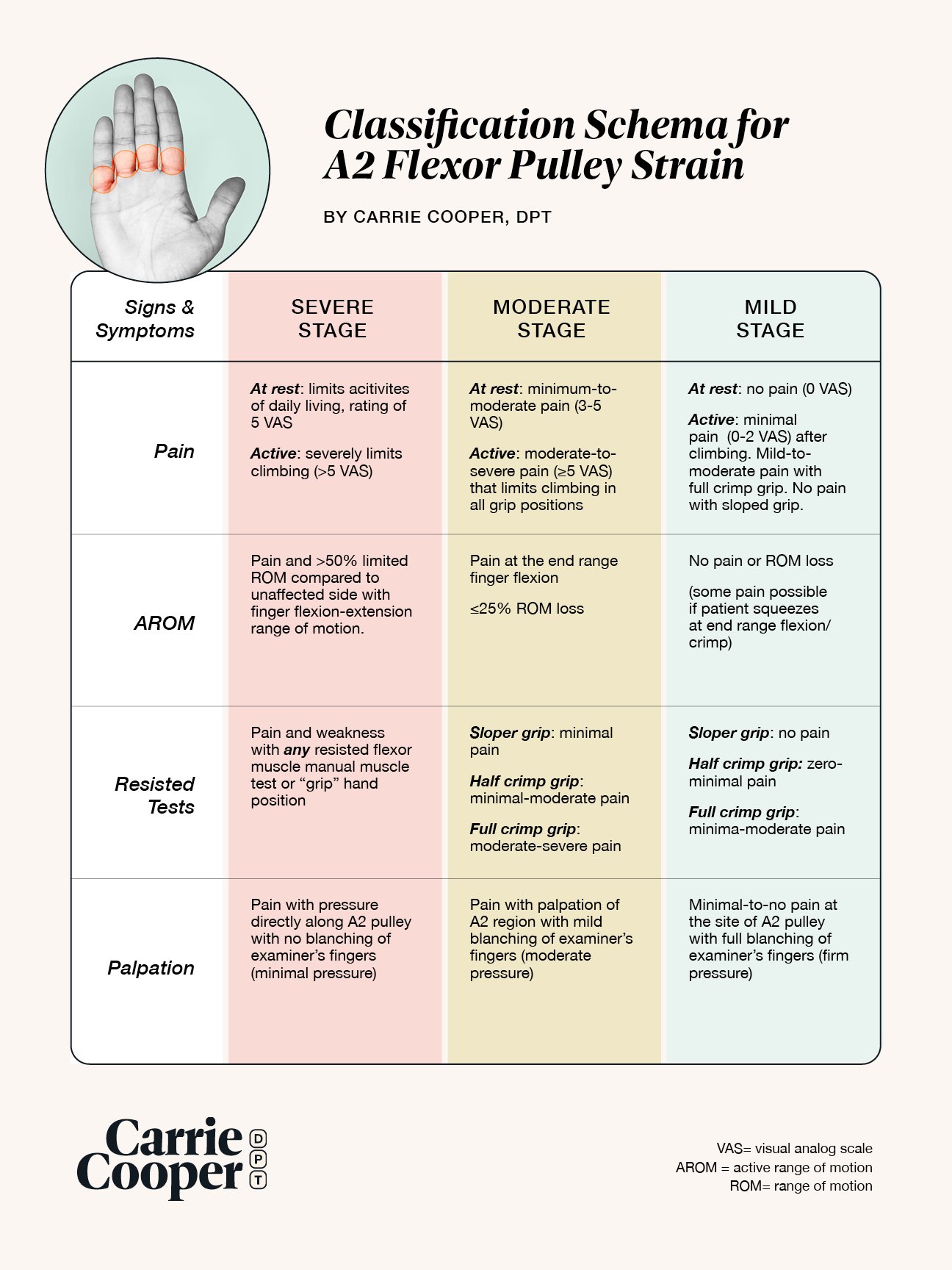
In 2020, we published a new criteria to that uses a combination of pain level measurement, active and passive range of motion, resisted tests, and palpation in order to determine the severity of a pulley injury.
You can download a PDF (or even get a poster!) of the Cooper Classification Schema here.
Treatment Methods
-
A pulley protection splint is a custom splint made for the purpose of reducing the tendon bone distance while the pulley is healing (See Fig 3A). It is an orthotic customized to protect the pulley by applying a compressive force, while also minimizing pressure to the nerve/artery/veins on the sides of the finger. It is different from just a circumferential taping in that its main purpose is to compress the tendon to the bone while allowing for normal function of other anatomical components. Because it is worn over a period of weeks, the orthotic is preferred over H-Tape to minimize irritation of the skin (though skin irritation may still occur).
For a severe pulley injury, a custom-made PPS by a hand therapy specialist is recommended.
-
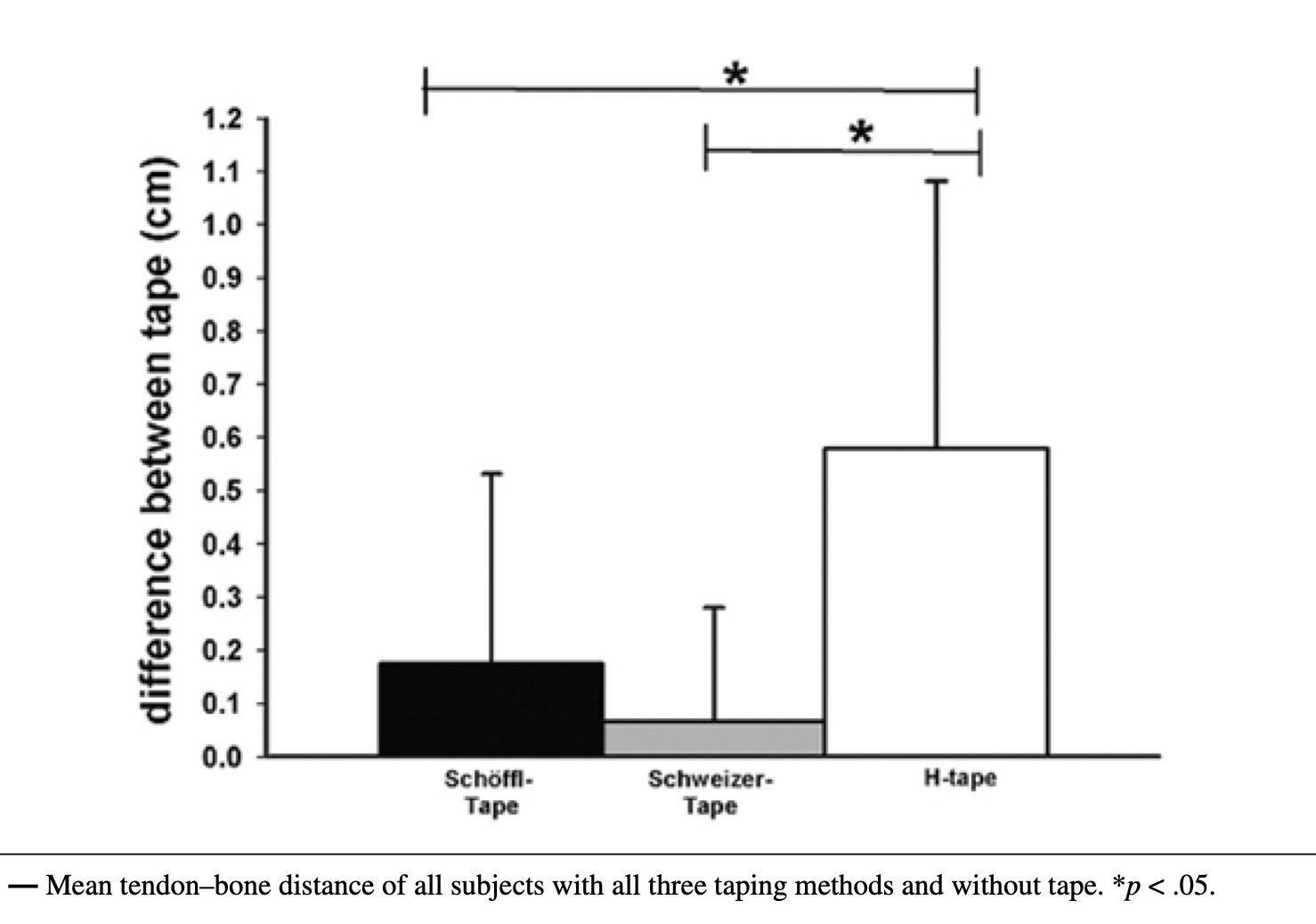
H-Tape is a therapeutic taping method that applies a sustained force directly over the PIP joint (see Fig 3B). By dividing the tape into two distinct strips with a bridge in the middle, the force can more effectively be transmitted directly to the area of the finger where the distance between tendon and bone is the greatest with a pulley injury. It has been shown in peer reviewed studies to outperform other taping methods (see Fig 3C).
For a severe pulley injury, a PPS is preferable over H-Taping because it’s designed to be worn over a long period of time. Tape loosens up and irritates the skin, making the wearer less likely to continue using it when these symptoms arise. There is no known study showing that people will wear the H-Tape for the desired amount of time required for full pulley healing.
Learn more about H-taping here.
-
Friends don’t let friends buddy tape and climb!
Buddy taping connects one finger to the other and is a signal to the body that a finger is injured, but it does nothing to protect an injured pulley. It does not support or protect the figure while it heals. What is does do it teach it to rely on the closest ally and get even weaker while further eluding the healing process.
Pen Rolls/Flexor Tendon Flossing:
If you do not have pain with any grip positions, this is a great exercise for using the musculotendinous unit throughout its range of motion, but for climbers, this is not a rehab tool.


Got a finger injury?
Figure out what’s going on and what to do about it using our self-assessment tool.